When a scrap-metal fire erupted in Camden in February 2025, smoke blanketed the city for hours. The air felt heavy and poisonous as the odor seeped through windows and walls. Residents used anything they could find to cover their faces, waiting for the haze to pass.
Most of us in Camden felt the respiratory danger that day. Many knew our lungs were at risk, but few realized that the same smoke may also have been silently harming our eyes.
Dry Eye Disease (DED), once dismissed as a minor irritation of aging or allergies, is increasingly recognized as a condition driven by environmental toxins.
Research across continents has linked exposure to airborne pollutants such as fine particulate matter, nitrogen dioxide, and ozone with higher rates of eye irritation, inflammation, and tear-film instability.
Camden, surrounded by major highways and industrial sites, faces fine particulate matter concentrations above the state average year-round. Levels spike to dangerous extremes during industrial incidents like the multiple EMR fires.
These pollutants don’t just cloud the sky; they infiltrate the body. They damage organs, including the eyes, robbing people of comfort, vision, and quality of life.
Dry Eye Disease affects roughly one in nine people worldwide, causing burning, tearing, redness, and blurred vision. But for those in polluted urban centers like Camden, it is more than a nuisance. It’s inequality.
The condition follows a self-perpetuating cycle: an initial insult triggers cell death and inflammation that destabilizes the tear film, causes dryness, and leads to more inflammation. DED can disrupt concentration and productivity in the workplace, impact social and physical functioning, and worsen overall quality of life.
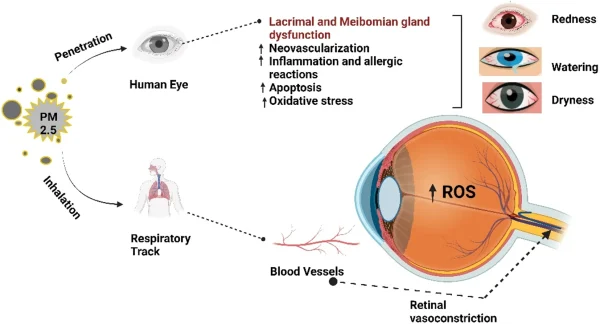
Airborne pollutants are potent initiators of this cycle. Their microscopic size allows them to reach the ocular surface, where they disrupt normal tear production.
Recent studies show that nitrogen dioxide exposure worsens ocular symptoms and destroys protective cells in the eye. Ozone at the ground level leads to chronic inflammation. Rising fine particulate matter levels worsen ocular discomfort, tear instability, ocular damage, and show the strongest association with Dry Eye Disease severity among air pollutants.
In Camden, where annual fine particulate matter levels are among the highest in the state, every flare-up of smoke amplifies this risk.
During the EMR fire, South Camden recorded a daily average that was about five times the annual average for Camden. Hourly readings reached levels that were roughly 50 times higher than the U.S. annual average.
Camden residents live with chronic exposure punctuated by extreme events, and the result is an invisible epidemic of ocular inflammation. In the story of environmental injustice, the eyes have been overlooked.
To be sure, research on air pollution’s impact on eyes faces challenges. Studies differ in methodology, symptom measurement, and pollutant tracking. Human exposures are difficult to isolate and standardize. And Dry Eye Disease itself can stem from multiple causes: aging, autoimmune disorders, medications, or trauma.
Nevertheless, the scientific consensus is growing that air pollution is a modifiable risk factor for eye disease. We may not be able to slow aging or alter genetics, but we can limit emissions, reduce patient exposure, and strengthen environmental regulations.
Ocular and systemic inflammation in Camden are not coincidences; they are consequences. Clinicians and patients should treat air quality as an eye-health issue. Untreated Dry Eye Disease can progress to chronic pain, corneal damage, and vision changes.
Environmental-related dry eye in Camden requires action now.
Healthcare providers and patients alike can monitor air quality via phone apps such as AirNow, a government-developed app. By monitoring air quality for high levels, users can limit time outdoors and reduce their risk of environmental DED.
Reducing Camden pollutant levels is the only cure for this inequity. Lawmakers are actively working to address this issue. However, public health agencies should integrate ocular health into pollution-exposure alerts, and local education campaigns can help residents recognize that “bad air days” are also “bad eye days.”
The next time Camden experiences a pollution crisis, we shouldn’t just worry about breathing. We should worry about seeing.
Roger Sheffmaker is a medical student in Camden. The ideas expressed in this article are his own and do not reflect the views of Cooper Medical School or Cooper University Hospital.